
You tried one medication, then another, and continued taking different antidepressants. No results? You adjusted doses, switched classes, added augmenters. You waited six weeks, then eight. Nothing held!
Treatment-resistant depression is not a character flaw, it is a biological mismatch between standard antidepressants and the specific neurobiology driving your symptoms.
Ketamine for treatment-resistant depression works through a different mechanism than every SSRI, SNRI, or atypical you have ever taken. It targets the glutamate system, triggers rapid synaptic repair, and can produce measurable relief within hours, not weeks.
By submitting this form you agree to be contacted via phone/text/email.
At Ketamine Wellness New York, we treat TRD patients who hcave exhausted standard options. This guide explains how IV ketamine works, what the clinical evidence shows, and whether you may be a candidate.
Let’s first define TRD precisely. The clinical threshold matters both for understanding your diagnosis and for deciding whether ketamine infusion for depression is the right next step.
The STAR*D trial is the largest study ever conducted on antidepressant outcomes. Its findings reshaped how we understand the limits of standard pharmacotherapy.
According to a study in the American Journal of Psychiatry, only about 28% of patients achieve remission on their first SSRI. By the fourth medication attempt, 33% of patients still have not achieved remission.
This is not a failure of will. It is a biological ceiling on what serotonin-targeted drugs can accomplish for a significant subset of patients. If you are in that third, standard pharmaceutical pathways were never going to be enough.
Understanding why traditional antidepressants have their limits is not just academically useful. For TRD patients, it resolves a years-long question: Is something wrong with me, or with the drugs? This section addresses the neurobiology behind medication failure.
The “chemical imbalance” framing, the idea that depression simply means low serotonin, is incomplete. For many patients, depression involves the glutamate system, measurable BDNF deficiency, and physical loss of synaptic connections in the prefrontal cortex and hippocampus.
SSRIs increase serotonin availability. For patients whose depression is rooted in serotonin dysregulation, this works well. For patients with glutamate-driven, structurally-mediated, or neuroinflammatory depression, increasing serotonin does nothing.
This is a mechanism mismatch, not a personal failure. Ketamine for depression in NYC addresses this by targeting glutamate directly, the system SSRIs simply cannot reach. Here’s a comparison of ketamine vs. SSRIs, focusing on which one acts faster.
Research shows that chronic stress and persistent depression reduce dendritic spine density in the prefrontal cortex. This means the actual physical connections between neurons deteriorate.
A serotonin boost cannot rebuild a synapse that no longer exists. This is why, for some TRD patients, the problem is not chemistry, it is structure. The brain’s wiring has been compromised, and the treatment needs to restore it.
This is where ketamine therapy NYC differs from every antidepressant class available. The mechanism is not incremental, it is categorically different. Understanding it explains why patients with years of treatment failure can experience rapid relief.
Ketamine works as an NMDA receptor antagonist. By blocking NMDA receptors, it triggers a rapid increase in glutamate activity at AMPA receptors. This glutamate surge is what initiates ketamine’s antidepressant effect, a pathway that serotonergic drugs never access.
The AMPA activation drives the release of Brain-Derived Neurotrophic Factor (BDNF). Think of BDNF as the structural repair signal for neurons. It supports the growth and maintenance of synaptic connections that chronic depression has eroded.
This is not chemical masking but a structural restoration at the neural level. So, ketamine therapy at Ketamine Wellness NY helps rewire the neural architecture in hours, not weeks. Learn more about how ketamine promotes neuroplasticity and rapid brain rewiring.
In a study published in Science, researchers found that ketamine induces a rapid increase in dendritic spine density in the prefrontal cortex, within 24 hours of administration.
The brain is physically rebuilding synaptic connections in less than a day. This mTOR-dependent synapse formation is the structural basis for ketamine’s rapid onset.
This explains why patients who have been unresponsive to years of medication can feel a meaningful shift after their first few infusions.
Traditional antidepressants may produce modest synaptic changes over months. Ketamine produces measurable dendritic growth within 24 hours. This timeline difference is not marketing, it is the clinical mechanism behind the response rates.
Not all ketamine delivery methods are equivalent, especially for treatment-resistant depression. Here, we’ll compare the three main pathways so you can have a meaningful conversation with your provider.
The differences in bioavailability and oversight are clinically significant for high-acuity TRD patients.
| Feature | Ketamine Wellness NY (IV) | Spravato (Esketamine) | At-Home Ketamine (Oral) |
|---|---|---|---|
| Bioavailability | 100% (Maximum) | ~30–50% (Moderate) | ~17–24% (Low) |
| Dosing Precision | Clinically calibrated | Fixed nasal spray | Variable / sublingual |
| Onset Speed | Hours to days | Rapid to moderate | Slower (weeks) |
| Medical Supervision | Continuous, in-person physician | Required (2-hr post-dose) | Minimal to none |
| TRD Evidence Base | Extensive, including NEJM 2023 | FDA-approved for TRD | Not FDA-approved for psychiatric use |
| Safety Monitoring | Real-time vitals and airway | 2-hour observation | Self-monitored |
| Protocol Type | Personalized, racemic mixture | Standardized (S-isomer) | Unstandardized (compounded) |
Takeaway: For treatment-resistant depression, 100% IV bioavailability under physician monitoring is the highest-precision delivery pathway available.
At-home ketamine services have grown in accessibility, and for mild-to-moderate depression, some patients may benefit from them. But ketamine for depression at home is a different conversation when your diagnosis is treatment-resistant depression.
Here is the clinical reasoning, not a sales argument.
Research published in Psychopharmacology confirms that oral and sublingual ketamine delivers only 17–24% of the compound to the brain due to first-pass hepatic metabolism. At-home lozenges fall in this range.
For a patient with mild depression, a low-dose sublingual product may move the needle. For a patient who has failed six antidepressants and possibly TMS, that dose is not enough.
This is because it won’t trigger the glutamate cascade or BDNF release needed for meaningful neural repair. The dose required to treat TRD is simply not safely achievable outside a clinical setting.
This is not a clinical opinion but a regulatory fact. The FDA has issued a safety communication warning that compounded at-home ketamine is not FDA-approved for psychiatric conditions and lacks the necessary in-person monitoring for patient safety.
TRD patients often carry comorbid conditions, complex medication regimens, and CVS risk factors that require real-time clinical oversight.
The therapeutic experience itself, a dissociative state at clinical doses, requires a safe, supervised container. That cannot be replicated in a home environment.
Many patients ask about Spravato (esketamine) before or alongside their IV ketamine inquiry. Both are real options. We explain them without dismissing either because the right choice depends on your specific clinical history and treatment goals.
Spravato contains the S-isomer of ketamine, which is delivered intranasally. It is FDA-approved specifically for TRD and is often covered by insurance, a meaningful practical advantage. Its bioavailability runs roughly 30–50%.
IV ketamine uses the racemic mixture, both the S and R isomers, delivered directly into the bloodstream at 100% bioavailability. The evidence base for IV ketamine predates Spravato by decades.
Some clinicians and patients find that the racemic IV mixture produces more durable results, particularly for those who have not responded to Spravato.
Neither is categorically “better.” They are different tools. At Ketamine Wellness NY, we help you understand which pathway aligns with your history and coverage situation.
“The patients I see with true treatment resistance have often tried Spravato or a prior ketamine program and experienced partial, but not sustained, relief. In many of these cases, the shift to a personalized racemic IV protocol with precise dosing calibration produces a qualitatively different response. The bioavailability gap and the dosing control are not small variables when you’re treating someone who hasn’t responded to anything else.”
Knowing the process reduces anxiety and sets accurate expectations. This section walks through the specific steps we follow for ketamine infusion depression patients at our Queens and Long Island clinic, from initial screening to maintenance.
The initial consultation is clinically thorough. Dr. Qureshi reviews your full antidepressant history: which medications, at what doses, for how long, with what side effects.
We evaluate previous interventions, i.e., TMS, ECT consultations, psychiatric hospitalizations, and any prior ketamine exposure.
Medical screening covers cardiovascular fitness, current medication interactions, and any contraindications. Patients with active psychosis, uncontrolled hypertension, active mania, or current high-dose benzodiazepine use require evaluation before proceeding.
The standard TRD protocol is six IV infusions administered over two to three weeks. This frequency is not arbitrary and builds a cumulative effect, reinforcing new synaptic connections before they can fade between sessions.
Each session lasts approximately 40–60 minutes of active infusion time, followed by a brief recovery period. Vitals are monitored continuously throughout.
Maintenance is individualized. Some patients achieve sustained remission and return only for quarterly boosters. Others integrate regular maintenance infusions into an ongoing treatment plan alongside psychiatry and therapy.
We do not replace your existing psychiatric relationship. We work alongside your prescriber to ensure ketamine therapy amplifies, rather than disrupts, your broader mental health care.
Here’s our detailed guide on why antidepressants stop working and how ketamine can be a savior when everything else fails.
TRD patients have been over-promised results across years of treatment. We will not add to that history. This section states the evidence clearly, including what ketamine cannot guarantee.
A 2023 trial published in the New England Journal of Medicine compared IV ketamine directly to ECT in 403 TRD patients.
Ketamine showed a 55% response rate compared to 41% for ECT, with significantly fewer memory-related side effects. This is a landmark comparison, ECT is considered one of the most effective interventions for severe depression.
A 2020 systematic review and meta-analysis in the Journal of Affective Disorders found consistent evidence of IV ketamine’s efficacy across TRD trials, supporting response rates in the 50–70% range.
Roughly 30% of TRD patients do not respond meaningfully to ketamine. We state this directly. The provider who is honest about limitations is the provider you can trust with your care.
For those who respond, the experience is often described as a lifting of weight, a sudden ability to engage with therapy, relationships, and daily function that depression had blocked.
Some patients achieve full remission. Some achieve partial but meaningful improvement that allows other therapies to finally take hold.
Responders often describe changes not just in mood but in the quality of their cognition. They report sharper thinking, reduced cognitive fog, and a reconnection with a sense of self that depression had eroded. These are the outcomes we aim for at Ketamine Wellness New York.
Candidacy is nuanced, and the consultation is where we assess it properly. The evaluation framework follows the American Psychiatric Association’s published consensus on ketamine use in mood disorders.
These guidelines give you a starting framework for understanding whether ketamine for TRD may be clinically appropriate for you.
These are starting points, not hard rules. The candidacy assessment with Dr. Qureshi reviews your full clinical picture before any recommendation is made. We do not treat patients who are not appropriate candidates, and we explain why clearly.
Cost is a real factor, and we address it directly. But for TRD patients, the economics of ketamine therapy deserve context because treatment resistance carries its own cumulative financial weight.
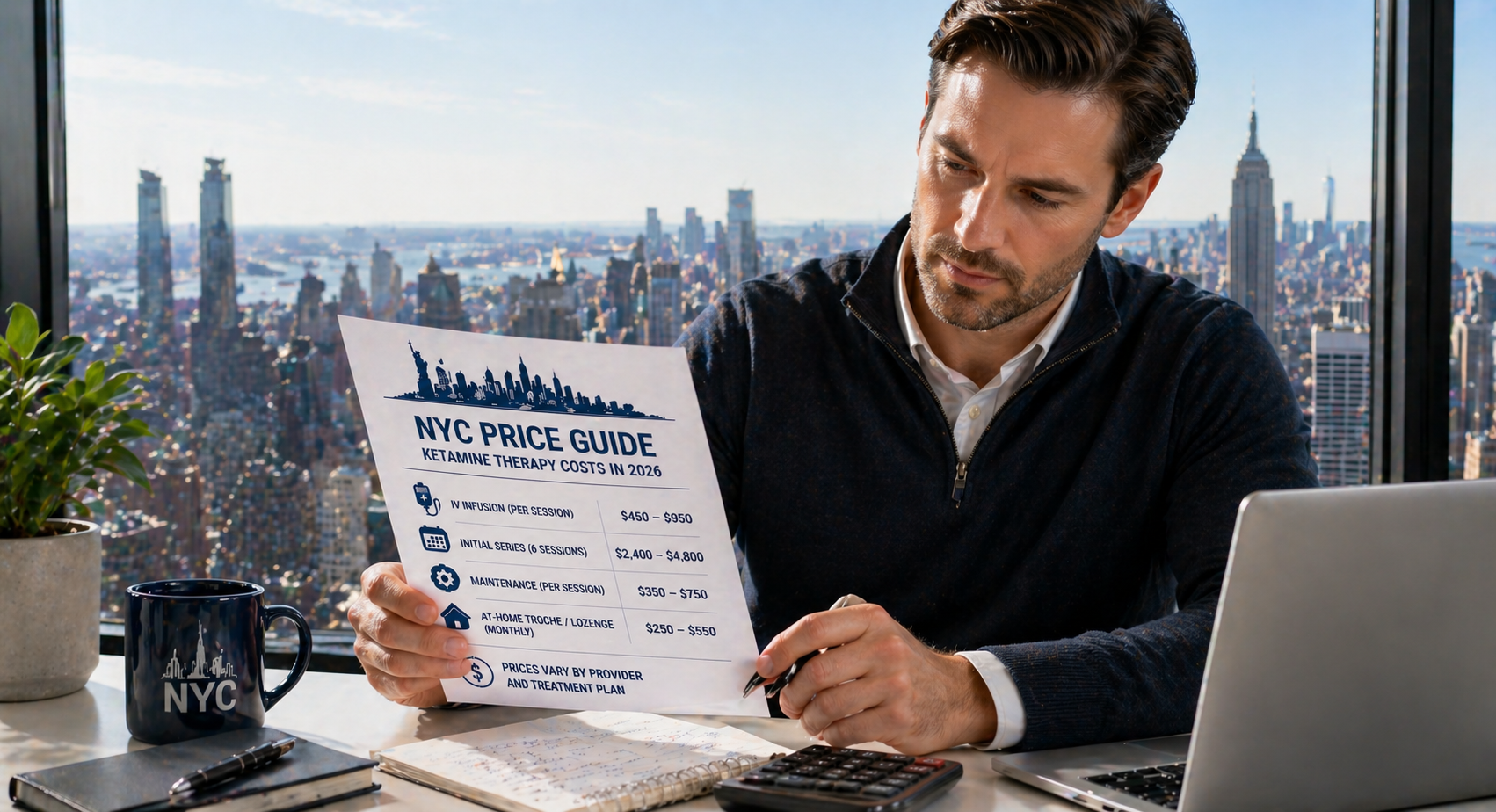
Our current pricing for ketamine for depression NYC:
Consider what TRD has already cost. Failed medication trials involve months of side effects, dose adjustments, and ongoing psychiatry appointments.
A TMS course typically runs $10,000–$15,000 out of pocket when not covered by insurance. Lost workplace productivity, modified career trajectories, and reduced quality of life represent an economic burden that rarely appears in the treatment cost column.
A six-infusion induction at $3,150, against a 50–70% response rate in patients with exhausted standard options, represents a relatively modest incremental investment.
Many patients who reach us have spent this amount or more in a single year of conventional psychiatric care without comparable results.
Clinical-grade IV ketamine for TRD is not a commodity service. The quality of the oversight, the precision of the protocol, and the clinical depth behind candidacy decisions all affect outcomes. Here is what distinguishes our approach for TRD patients specifically.
TRD is defined as failure to achieve symptom relief after at least two antidepressant trials of different medications at therapeutic doses for six to eight weeks each. This helps distinguish true TRD from cases where trials were cut short due to side effects or inadequate dosing.
Unlike oral antidepressants that take weeks, IV ketamine can produce measurable mood improvement within hours to days. Most TRD patients notice meaningful change between their third and fifth infusion in the six-session induction series.
Yes, IV ketamine is given in a controlled medical setting with continuous monitoring of heart rate, blood pressure, and oxygen levels. The FDA has warned that at-home compounded ketamine lacks required in-person monitoring for safe psychiatric use.
Mostly, yes. Ketamine acts on the glutamate system, while antidepressants target serotonin or norepinephrine, so they can often be used together safely. Our medical team reviews your medications during consultation to confirm compatibility and adjust timing if needed.
A single infusion is not enough to evaluate TRD response. The six-infusion induction series builds cumulative neural repair effects. Most responders improve between sessions three and six, and completing the full protocol is clinically essential before assessing outcomes.
If standard antidepressants have not worked, that is not a verdict on your future. It is a signal that the treatment approach needs to change, not that treatment cannot work.
IV ketamine for treatment-resistant depression offers a mechanism that serotonin-targeted drugs simply cannot replicate: glutamate modulation, rapid synaptic repair, and structural neural restoration within hours.
The evidence base is real. The response rates are meaningful. And for patients who have tried everything else, those two facts matter enormously.
Treatment-resistant depression varies patient to patient. The consultation is how we determine whether IV ketamine aligns with your specific treatment history, current medications, and clinical situation. No pressure, just a clinical conversation.
Schedule A Candidacy Assessment

Standard treatments for alcohol use disorder help many people. But relapse rates remain high, and

Complex regional pain syndrome (CRPS), also known as reflex sympathetic dystrophy (RSD), sits among the

The infusion ends, the IV comes out, and you start to feel like yourself again.

Ketamine For Sleep: What NYC Patients Should Know Poor sleep is exhausting in ways that

Note: Names and identifying details have been changed to protect patient privacy. Stories reflect documented

Note: Names and identifying details have been changed to protect patient privacy. Stories reflect documented

The wait is the hardest part. Anxiety makes sleep impossible. Every stressor triggers a physical

Panic disorder does not just feel scary. It quietly reorganizes your entire life around avoidance.
You tried one medication, then another, and continued taking different antidepressants. No results? You adjusted

The room is dark. The blinds are shut. Even soft light sends pain radiating behind

The burning never fully stops. It’s there when you wake up, when you try to

The cost of a single IV ketamine infusion in 2026 typically falls between $400 and
You did the work. You spoke with your psychiatrist, gathered your medication history, submitted the

If you have an Aetna plan and you’re considering ketamine therapy for depression in New

Ketamine therapy, particularly in the form of intravenous (IV) infusions, has become a go-to treatment
Living in New York City often means paying a premium for everything, from rent to

For many individuals living with obsessive-compulsive disorder (OCD), the mind feels like a transmission with

Ketamine therapy is gaining popularity for its ability to alleviate severe depressive symptoms in hours

Finding affordable mental healthcare in New York can feel like navigating a maze, especially when

For many, therapy offers a vital path to healing and self-discovery. However, after years of
Thank you for choosing Wellness Clinic. Our specialist care team will contact you within the next 12 hours to confirm your appointment and answer any questions youmay have.
our team will review your message and contact your shortly. we look forward to supporting your wellness journey
Check your phone or email to receive your unique coupon code. You’ll need it when booking your first appointment.
